
Do vaccines cause autism?
Origins, data, solutions.

It was recently claimed by Reuters that the CDC, under the stewardship of the newly appointed HHS Secretary Robert F Kennedy Jr, is planning a new study into the potential link between vaccines and autism. The overwhelming response from my scientific colleagues was one of condemnation and disparagement. Some decry the negative impacts of giving legitimacy to “anti-vaxxers”. Others laugh at the juxtaposition of DOGE trying to slash government spending whilst HHS wastes funds on something that is well-settled. There were some pretty funny responses actually.

Whilst it’s very popular to dunk on MAGA these days, I think it is worth giving more sincere consideration to the predicament we find ourselves in with regards to health policy and public trust in science in the post-COVID era.
There is a need for scientists, politicians, and commentators to empathise with the members of the public who distrust the expert class. The thing is, this distrust isn’t random. It was completely deserved. The expert class spent the last five years lying to the public again and again. This included lies about the efficacy of masks, the efficacy of vaccines, the lack of efficacy of alternative COVID treatments, and lies about the origins of COVID. All the while, inflation disproportionately ravaged the poor, the rich got much richer, and Big Pharma basked in their unprecedented legal protections and government-mandated profits in complete absence of real free market forces.
To dismiss skeptical members of the public as moron anti-vaxxers is not only the opposite of helpful, but demonstrates a supreme lack of empathy and surplus of narcissism—driven by the good feeling that one gets when proving the out-group wrong and oneself right, intelligent, and moral. What’s more, much of the credentialed elite are often too arrogant to even attempt to interrogate the claims of people less educated than themselves—dismissing them out of hand because of who the claims are coming from, rather than because of what the claims are. We’re left with an ecosystem where the experts aren’t really experts, but just parrots of dogma. Meanwhile, the distrusting public aren’t being engaged in good faith, but instead reprimanded for questioning the dogma. Resultantly, they are browbeaten downwards into theories of conspiracy.
Truth and honesty is the cure to all of this. So what is the truth when it comes to vaccines and autism? To understand how we got here, we should go back to the origin of the vaccines-cause-autism story. We must go back to the academic fraud of Andrew Wakefield.
The Lancet paper
In 1998, a team of physician-scientists from the Royal Free Hospital in London, UK, published a paper in The Lancet that is now often considered the seed of the vaccine-autism hypothesis. The infamous paper is a rather simple case report that described and attempted to explain the symptoms of twelve children who all seemed to suffer from the same syndrome. Here is the introduction to the report in full:
We saw several children who, after a period of apparent normality, lost acquired skills, including communication. They all had gastrointestinal symptoms, including abdominal pain, diarrhoea, and bloating and, in some cases, food intolerance. We describe the clinical findings, and gastrointestinal features of these children.
Many of the authors, including first author Andrew Wakefield, were gastroenterologists, and gastrointestinal symptoms were the primary focus of the paper. It was the parents of the children who drew the link with the MMR vaccine, with parents of eight of the twelve reporting to the doctors that onset of symptoms quickly followed MMR vaccination (some as soon as 24 hours post-vaccination, others up to two weeks post-jab). One of the other four kids had been infected with measles itself, another had recurrent ear infections, and the parents of the final two didn’t report any coincidences that they had noticed leading up to onset of the syndrome.
The doctors included these parental observations in their study and added a table which included time between MMR vaccination and symptom onset for all twelve children (including the ones whose parents had not made the link themselves). The researchers went on to investigate the gastrointestinal symptoms, performing endoscopies, histology, and urinary analysis. Broadly, they showed signs of chronic inflammation in many of the children’s gut linings, but no signs of bacterial infection. They do no further analysis to explain the neurological symptoms of the children (primarily autism), but connect the dots between their twelve cases and the literature at the time in stating there seems to be a real link between issues in the gut and issues in the brain. The link between gastrointestinal issues and psychiatric disorders has been definitively corroborated by decades of further research, with scientists even proposing modulation of the gut microbiome (via pre/probiotics or fecal microbiota transplantation, for example) during early life as a potential preventative measure against autism.
Whilst the existence of the gut-brain-axis did used to be a fringe area of medical science and was pooh-poohed as pseudoscience for much of the 20th Century, discussing this connection wasn’t what got the paper retracted and Wakefield’s medical license revoked. Most know what I learned in A-level biology class: that it was retracted because of the fake data used to claim that vaccines cause autism. So where and how did they make this claim? I had never read the paper itself until a couple years ago, when I was surprised to find out that, actually, the authors make no such claim.
If your goal is to combat pseudoscience (valid) and publicly dunk on antivaxxers (tempting but ultimately self-serving), being wrong about Wakefield et al, 1998 is not going to serve you well. In actuality, the paper makes no causal claim regarding MMR vaccinations and autism. It doesn’t even claim an association. Indeed, it clarifies as much:
We did not prove an association between measles, mumps, and rubella vaccine and the syndrome described. Virological studies are underway that may help to resolve this issue.
Since the temporal coincidence of MMR inoculation and onset of symptoms for these twelve children was certainly notable, the authors do go on to speculate how investigating such a link should be carried out, and why it might be a valid hypothesis mechanistically, based on the literature available at the time. It’s probably worth noting here that the coincidence of symptom onset post-vaccination, whilst interesting, could simply be just that—a coincidence. Autism happens to appear during early childhood, which is the same period during which we choose to vaccinate humans for maximal efficacy.
One of the arguments people tend to make when questioning the link between vaccines and autism is that an increase in incidence of autism occurred in the years after MMR was introduced. Yet Wakefield et al cite literature pointing to the fact that actually there was no strong evidence of an increase in autism prevalence at the time. Indeed the apparent increase in prevalence to this day may simply be a result of broadened diagnostic criteria, increased surveillance, incentivised diagnosis, and even immigration of predisposed populations. Wakefield et al also cast doubt on a suggestion of a causal link, which might be inferred from their case report, by citing a 1997 epidemiological paper which analysed a large cohort of children and found zero association between measles vaccination and neurological side effects.
Wakefield et al go on to discuss potential genetic factors that have been associated with autism, namely the C4B gene which encodes a component of the complement system—part of the innate immune response. They discuss the perfectly salient point that a genetically impaired innate immune response could increase the likelihood of an adverse reaction to viral infections or attenuated virus inoculations (the basis of many vaccines). Since they found evidence of a vitamin B12 deficiency in urine samples from the children, they also suggest that this could contribute to autism—a hypothesis that is backed up by recent evidence.
I can’t believe I’m writing this, but … the 1998 Lancet paper is actually not bad. Decent even. It doesn’t overstate its claims; it speculates sensibly in the discussion section (this is the point of a discussion section) whilst citing high quality literature; and it pre-emptively caveats any implication that vaccines could cause autism. So why was it retracted?
The cracks begin to show
In the years following the paper’s publication, there was a slew of back and forth publications, each leaning one way or the other. For example, a serological study showed a link between a measles immune response (which could be produced by either vaccine or infection) and autoimmunity in the brain of autistic children. On the other hand, epidemiological evidence, though often underpowered, argued no association between MMR and autism.
Pressure was put on the Lancet, the Royal Free Hospital, and the UK General Medical Council to squash the hypothesis put forward by Wakefield and others, both in light of the disproving epidemiological correlations, and a decrease in vaccine uptake which many blamed on Wakefield.
Notably, MMR uptake was already on the decline before Wakefield’s paper, and insisting Wakefield was the cause here ironically falls foul of the same correlation-causation fallacy that critics accuse Wakefield of regarding vaccines and autism.
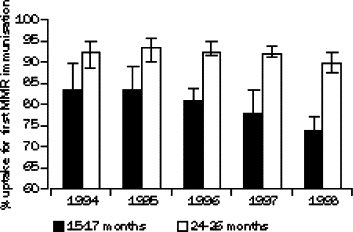
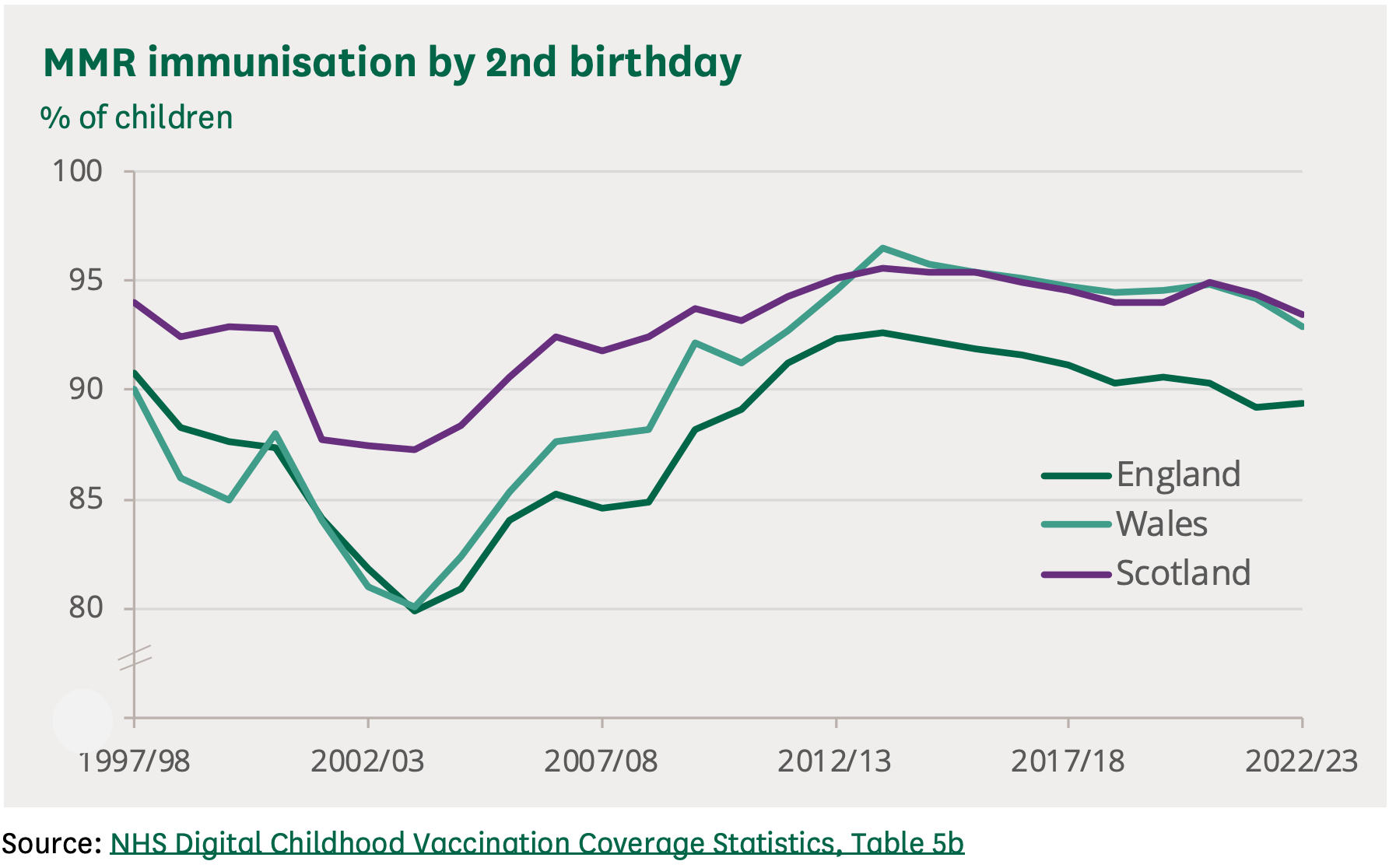
Additionally, an increase in uptake of the separate measles, mumps, and rubella vaccines coincided with the dip in uptake of the combined MMR shot—meaning total coverage was probably pretty stable over this period. Perhaps as a result, despite the frenzy, there was no real pubic health consequence post-Wakefield, with no notable increase in measles deaths post-1998. Indeed, there have been only nine deaths occurring in UK between 2000 and 2023 that could have been prevented by MMR vaccine (there was also one measles death in this time period in a vaccinated individual).
Amongst the panic and blaming, an investigation opened up into the validity—both ethical and scientific—of the Wakefield 1998 paper. It transpires that a group of lawyers, representing parents of perceived vaccine-injured children, had commissioned (i.e., were paying) Wakefield to perform a pilot study to gather evidence of a potential relationship between MMR and autism to be presented in their legal case. Some of the subjects in the 1998 Lancet paper were also used in this parallel study and neither this overlap nor the existence of the parallel study were disclosed by Wakefield in the original paper. Herein lied the first conflict of interest.
In 2004, The Lancet editorial board released a summary of the investigation, indicating that ethical approval for the study was valid, but that a conflict of interest should have been disclosed. Wakefield’s own statement argued that there was no actual conflict of interest, since he claimed that the two studies were separate, yet the Lancet editors rebuked that the “perception of conflict of interest” is what mattered, which I would agree with. There is no harm in declaring something that may or may not be an actual conflict of interest.
In this same 2004 issue of The Lancet, the Royal Free Hospital, its NHS Trust, and the UCL Medical School released a statement clearing Wakefield and co-authors of any medical malpractice, but indicating that key conflicts of interest should have been disclosed. Additionally, ten of the twelve authors (excluding Andrew Wakefield and Peter Harvey) published a “retraction of an interpretation”.
We wish to make it clear that in this paper no causal link was established between MMR vaccine and autism as the data were insufficient. However, the possibility of such a link was raised and consequent events have had major implications for public health. In view of this, we consider now is the appropriate time that we should together formally retract the interpretation placed upon these findings in the paper
As already discussed, these “major implications for public health” are fairly nebulous and non-existent. Nonetheless, clarifying the interpretation that these authors placed on their own work is a very useful practice, and surely would have helped prevent over-interpretation of the original paper (even though over-interpretation—in both directions—seems to be rampant to this day). As for Wakefield’s exclusion as an author of this statement, I can only imagine that he genuinely believed that vaccines could cause autism and so refused to take part in this clarification of interpretation.
The whole saga drew to a close in 2010, twelve years after publication, when the UK General Medical Council concluded their investigation and deemed Wakefield unfit to practice. They cited the conflict of interest already discussed, but also some patents Wakefield had filed for a proposed “treatment of an MMR virus mediated disease”. Again, nothing wrong with filing this patent, but failing to disclose it on the 1998 paper is the issue. Beyond these undisclosed financial conflicts of interest, the GMC also did find, contrary to the earlier investigation by the hospital itself, that appropriate ethical approval for all patient interventions was not acquired.
A few days after the GMC ruling, The Lancet issued a full retraction of the original paper, specifically because:
claims in the original paper that children were “consecutively referred” and that investigations were “approved” by the local ethics committee have been proven to be false
This disregard of ethical approval seems to be the real kicker, since failing to disclose conflicts of interests normally doesn’t result in retraction. At least, it didn’t for this 2011 editorial in the British Medical Journal titled “The fraud behind the MMR scare”, which itself failed to declare that the BMJ receives advertisement and sponsorship revenue from MMR vaccine producers Merck and GSK… oh the irony.
Ok science, bad scientist
My takeaway from all of this is that:
The actual findings of the 1998 paper are valid but minor contributions to the field and are fairly interesting
The 1998 paper was and is erroneously interpreted (by both sides) as arguing that vaccines cause autism, which it does not. Over-zealous journalists probably contributed to this distortion of interpretation (you don’t hate journalists enough… a topic for another time perhaps)
Wakefield cut corners and failed to disclose financial conflicts of interest, thus becoming his own worst enemy if he genuinely wanted to move the field to investigate neurological side-effects of vaccines.
So is there a link between vaccines and autism?
The best data we have come in the form of two very large retrospective cohort studies from Denmark—one in 2002, and the other in 2019. The 2002 study, published in the New England Journal of Medicine, looked at over half a million Danish kids, with around 82% of them receiving the MMR vaccine. The results report on the “adjusted relative risk” of autistic disorder or autistic-spectrum disorders.
For readers who are unfamiliar, a relative risk or hazard ratio of 1.00 means that there is neither an increase or decrease in risk associated with the intervention (vaccination here). Below 1 implies negative association (less risk), above 1 implies positive association (more risk). The 95% confidence interval (CI) describes the range that would contain the true RR/HR value in 95% of all possible random samples, if the sampling process were repeated many times. A bit confusing, but basically if the upper bound falls below 1, the negative association is considered to be statistically significant, whilst if the lower bound exceeds 1, a positive association is considered to be statistically significant. Below is the results table from the study:
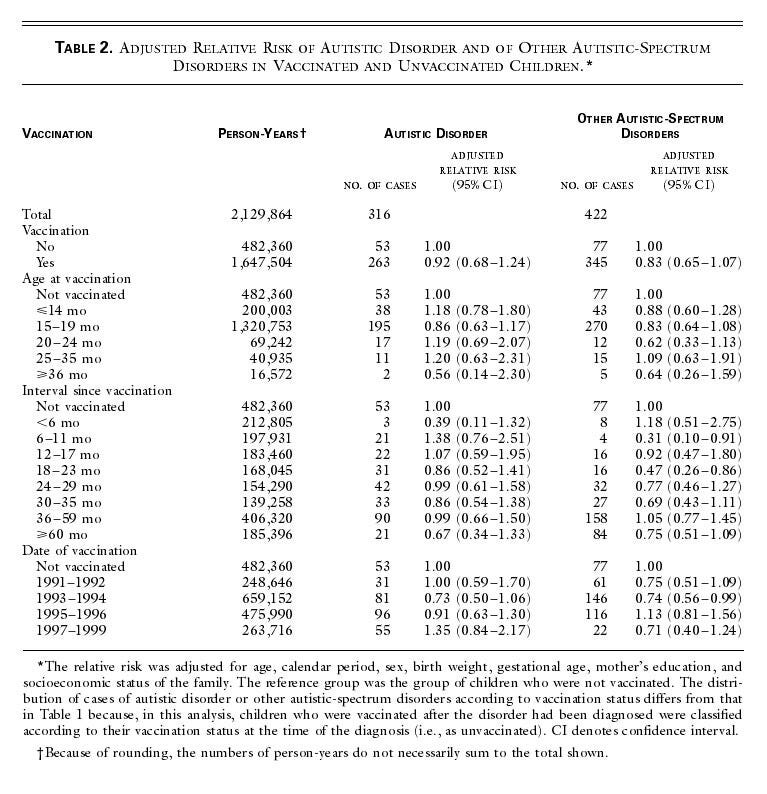
Whilst there was no statistically significant association between MMR vaccination and autism overall, binning the data by “interval since vaccination”, you can see that there is, in fact, a statistically significant negative association between MMR vaccination and autistic-spectrum disorders at 6-11 months (ARR = 0.31; 95% CI = 0.10 to 0.91) and 18-23 months (ARR = 0.47; 95% CI = 0.26 to 0.86) post-vaccination. This is fascinating. If the analysis is solid and the data are to be believed, this means that MMR vaccination could actually protect children from autism in these time windows! Is there a link between vaccines and autism according to this study? Yes. Yes there is. In the opposite direction.
If true, one explanation could be that the protection against the actual diseases decreases risk of autism. In such a scenario, the viral infection (but not vaccines) might promote autism—something seen in one of the children in the 1998 Wakefield case report who was infected with measles itself prior to autism onset. Alternatively, the vaccine could be suppressing autism via some other neuro-immune mechanism.
Okay, that’s interesting. Well maybe it was a fluke with this particular half million+ kids. Can we find a different or more statistically powerful study to compare?
Enter: the 2019 study. Published in the Annals of Internal Medicine, it was performed by the largely same group of scientists, and was an improvement of the first study. They used a non-overlapping cohort which was larger and they also followed up for longer. Additionally, they included analysis of subgroups at higher risk of autism based on environmental factors (e.g., if the mother smokes during pregnancy) and familial factors (a sibling with autism)—since failing to include these subgroups was a criticism of the first paper.
The headline result: no association (autism hazard ratio = 0.93; 95% CI = 0.85 to 1.02). You’ll note the upper bound of this confidence interval is pretty close to 1 though. When ending the followup at 3-years post-vaccination (the earliest they went this time), the aHR was 0.73 with 95% CI of 0.53 to 1.00—a borderline significant negative association.
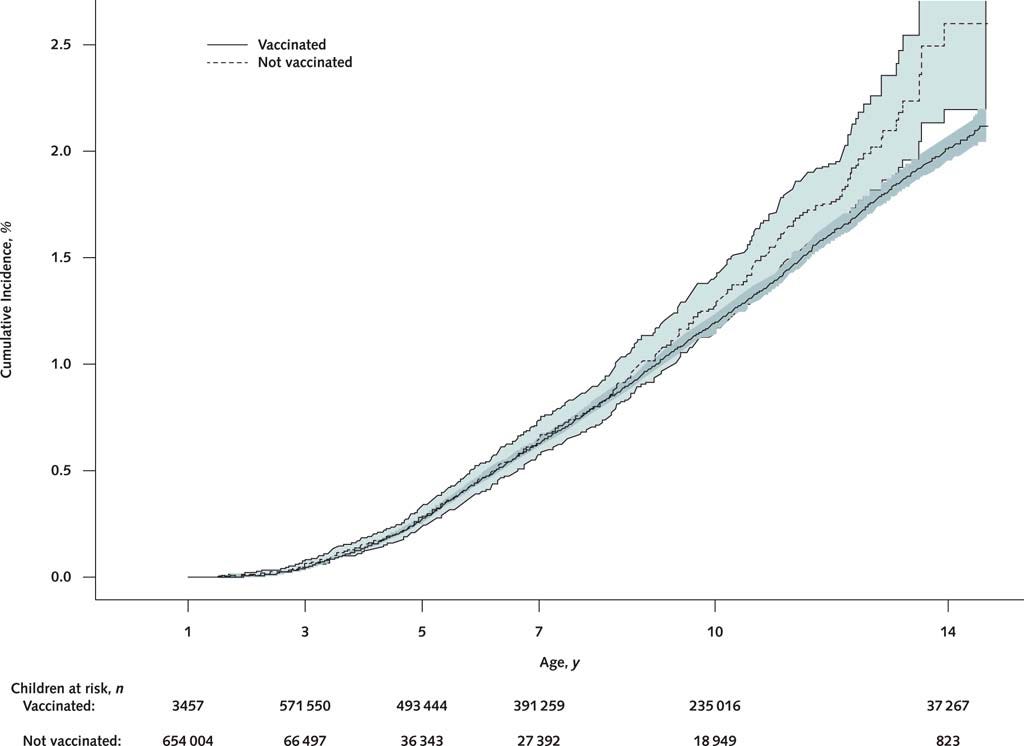
When plotting the cumulative incidence of autism, you can see that by age 14, the relative incidence of autism in the vaccinated group is significantly negative.
If the data are of both this and the 2002 cohort study are to be believed, then either we declare that vaccines might prevent autism, or we add caveats to our conclusions from the analysis. Sure—there is no positive association, but the analysis was two-tailed and evidence of a negative association is there. That’s just what the data show.
At the moment it just seems like the scientific and medical establishment choose to ignore this blip in the results, and are happy to conclude no association. I haven’t seen mention of it anywhere, least of all in the papers themselves. My suspicion is that the negative association is not a biologically real phenomenon, even though it is statistically significant within certain time windows. It could perhaps be explained by the adjustments for confounders (or lack thereof). Frustratingly (or not, depending on where you stand on this issue), the creation of a negative association out of thin air by failing to account for unknown confounders would, by the same logic, destroy any biologically real positive association.
This little blip in the data may seem inconsequential to most, or even helpful to the pro-vaxxers amongst us, but to me it is an amber flag. My personal opinion is that this is at least of interest and warrants further investigation. Surely Big Pharma, too, would be interested in a study looking into the prospect that vaccines might prevent autism.
Our best evidence could be stronger
It’s hard to know whether to believe the negative association seen in these studies or not. The solution (as always) is more research. There are three main reasons why we might be unsatisfied with the results of these large cohort studies:
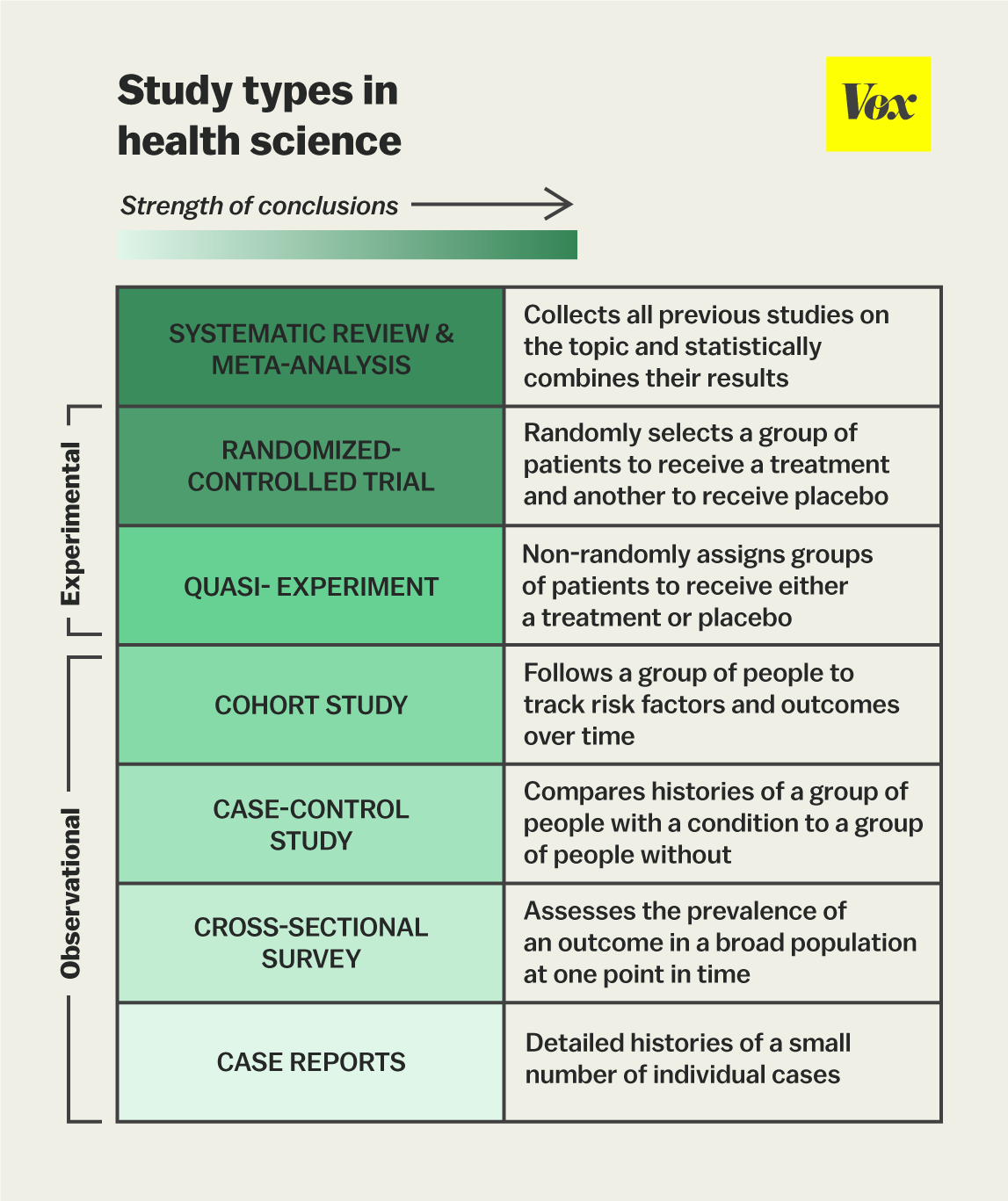
Large cohort studies are not appropriate for proving or rejecting causality. Biomedical studies can be designed in different ways, with certain methods of investigation more rigorous than others. Generally speaking, you want a large study where statistics can be applied to rule out happenstance results, and you want to eliminate bias or confounding variables as much as possible. In terms of proving causality, experimental studies are more powerful than observational ones (which can only show a correlation by definition). See the infographic below for the breakdown.
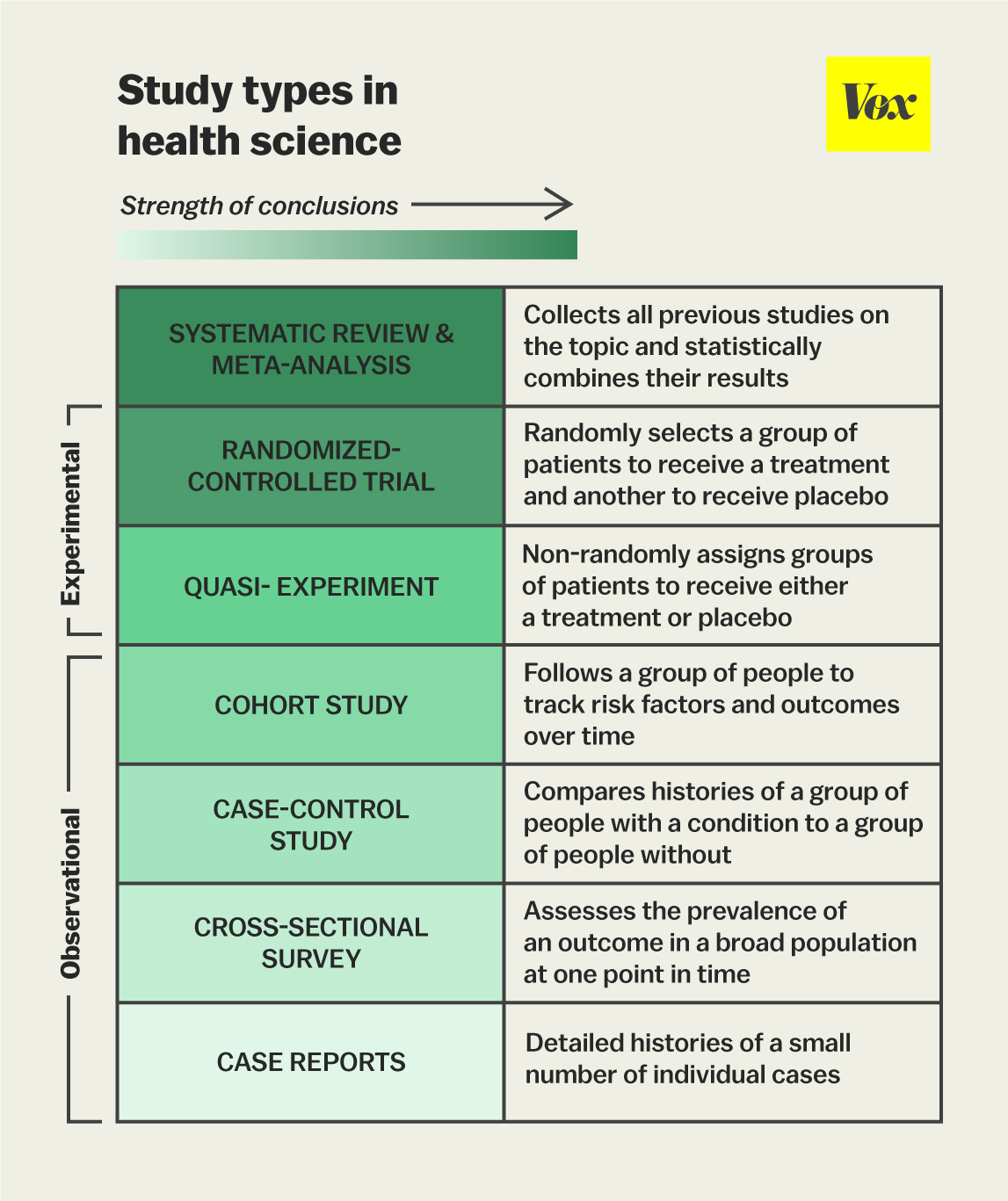
Note that the 1998 Wakefield paper was a case report, the least powerful type of study. Therefore anyone claiming that it proves anything simply doesn’t understand study design. Now these Danish studies, which are typically pointed to as the best evidence we have that MMR vaccination does not cause autism, are nation-wide cohort studies. They are also retrospective, meaning the specifics of analysis were figured out after the data were already out there. A prospective study, where analysis methods and parameters are decided upon before data collection, is slightly less prone to bias since you can’t hypothetically pick and choose stats tests to massage your data into giving your preferred result. Whilst they are pretty powerful (huge sample sizes), they are observational in nature and cannot offer strong conclusions about causality. A large randomised controlled trial would offer more conclusive results.
Studies are not always generalisable between nations. Given the well-established genetic inputs to autism, as we briefly covered earlier, comparisons of genetically distinct populations can be expected to produce different results. It is possible (though unlikely) that the Danes have fewer vaccine-triggered autism-associated genetic polymorphisms (if those exist at all…) than the English. The same is true for environmental inputs, including things like food supply, circulating infections, air quality, climate, etc., which all differ between countries. A specific but notable difference between countries is the vaccine schedule. The schedules differ between the UK and Denmark, for example. In the UK, doses are given at 12 months and then again at 3 years and 4 months (this booster was given at 4 years before 2013). Meanwhile, in Denmark doses are given later at 15 months and 4 years of age, with the second dose actually being given at 12 years of age pre-2008, when most data for both studies were collected. Giving doses at different stages of development might be expected to have different impacts. Thus, any positive or negative associations between autism and this vaccine schedule are simply not applicable to other vaccine schedules. Notably, the US vaccine schedule is an absolute Frankenstein’s monster compared to those of the Europeans.
Financial conflicts of interest. As we learned from the Wakefield scandal, conflicts of interest, particularly when undisclosed, are problematic. Even if scientists are aware of their own conflicts of interest, they can do little to combat any resultant subconscious bias. The 2019 study laudably disclosed funding from the Novo Nordisk Foundation. It’s pretty tenuous, but a potential issue arises here because the Novo Nordisk Foundation owns a controlling stake in Novo Nordisk (via its subsidiary Novo Holdings A/S). Novo Nordisk (via its subsidiary Novo Nordisk Pharmatech A/S) sells products to vaccine producers for their manufacture. So obviously painting vaccines in a good light would help Novo Nordisk Foundation and they’d be more likely to fund researchers amenable to their bottom line. I don’t actually think this impacted the studies, but it’s an obvious point of criticism for skeptics.
More research, not less
In general, I am a research maximalist. Truth and knowledge are my fundamental values. For this reason, I disagree with the recent decision to pull NIH funding for studies into transgender mice1. Equally, I see nothing inherently wrong with gain-of-function research2. Further, my primary emotional response to Jiankui He, of CRISPR babies fame, is inspiration rather than condemnation.
Hopefully we can acknowledge the lack of perfect certainty regarding any positive or negative association of MMR vaccination and autism based on our best studies, herein described. Hopefully we can also acknowledge the lack of generalisability acr
oss different countries and populations, and a paucity of very convincing evidence in the US specifically. In light of these acknowledgements, I think there are valid scientific reasons to support RFK’s supposed move to fund research into this, regardless of his personal motivations or hypotheses.
Politically, it also makes a lot of sense. If we assume, as many of us do, that vaccines have absolutely no positive or negative association with autism and that the immune system is largely uninvolved in its aetiology, we must acknowledge that there is a non-insignificant population of people in both America and elsewhere that are not as convinced as us enlightened ones. Allowing the most vaccine-skeptic administration in recent history to fund such research is the best possible chance we have to persuade everyone of the truth, whatever it is. An RFK-instigated, NIH-funded, pharma-independent, large, multi-centre, randomised control trial that conclusively shows no role of any vaccination in the development of autism would be the holy grail of silver bullets many of us are looking for to assure the skeptical public of the safety of vaccination. Dr Jay Bhattacharya, newly appointed director of the NIH, has said on the matter:
I don't generally believe that there is a link [between autism and vaccines] ... But what I have seen is that there's tremendous distrust in medicine and science coming out of the pandemic.
I have to say, I agree. I must end this essay the same way I started it—by asking “Do vaccines cause autism?” Let’s get the studies done.
I think that cross-sex hormones and gender reassignment surgery are pretty bad for the patients, based on the available evidence. As long as the science isn’t fraudulent and the results don’t get buried, more research providing evidence to back up or refute my current position here would be welcome.
In my view, the issue with origins of COVID-19 wasn’t GoF necessarily, but with the atrocious safety standards of the Wuhan Institute of Virology, the complete lack of accountability, and the massive international conspiracy and coverup. Science can be dangerous regardless of whether it involves gain-of-function. It’s also just an annoyingly provocative buzzword. I’m currently doing research to try to enhance the function of human T cells—that’s technically gain of function.